
Ear, Nose & Throat
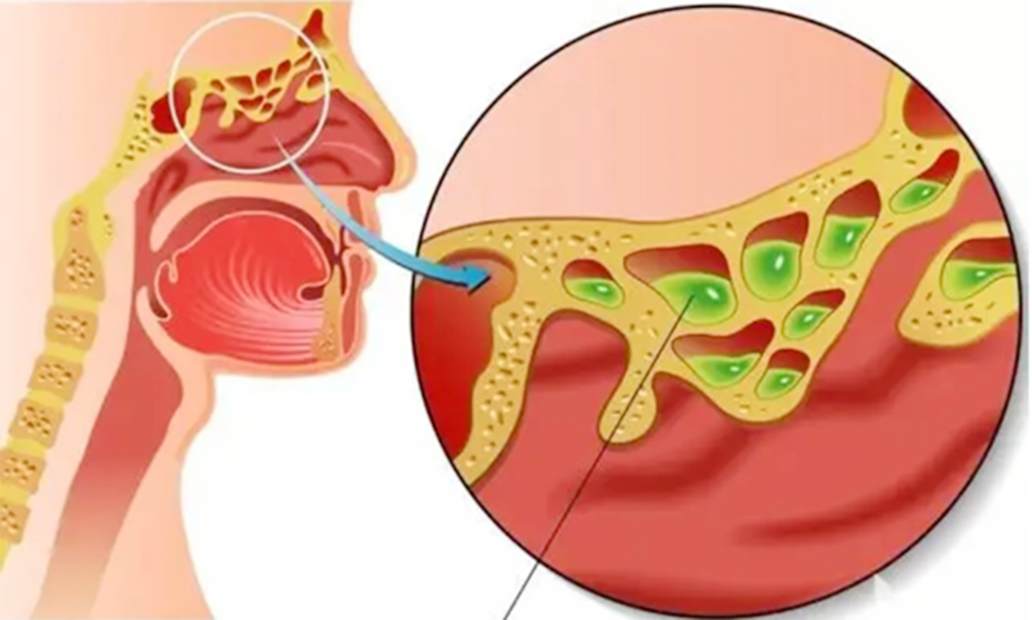


Sinusitis that has not been immediately treated or has not been completely cured, as well as by anatomical variations, bacterial and fungal infections, allergies, ciliary movement disorders, and iatrogenic factors. In addition, its onset is also closely related to genetic, environmental, and other factors.
Chronic rhinosinusitis is a common in ENT, head and neck surgery. According to a epidemiological survey, around 8 out of every 100 Chinese suffer from chronic rhinosinusitis.Chronic secretory otitis media is mainly caused by eustachian tube dysfunction, infection, immune response, and pressure damage.
Chronic suppurative otitis media is closely related to the persistence of acute suppurative otitis media, adjacent organ lesions, low immunity, and dysplasia of the mastoid process.
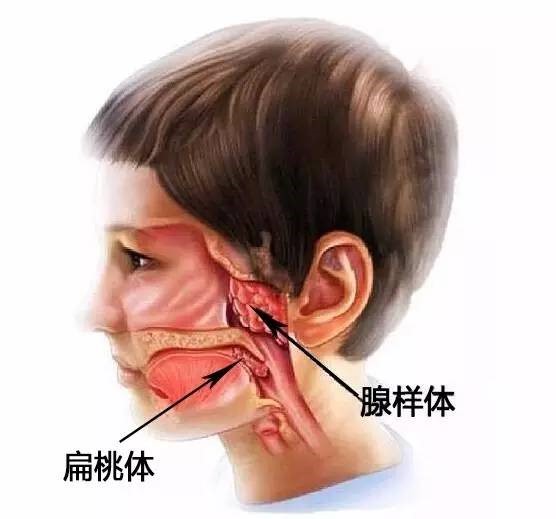
Secretory otitis media has a high incidence rate in children, which is one of the common causes of hearing loss in children.
According to foreign statistics, more than 50% of infants suffer from secretory otitis media, most of which recover within 3 months. According to statistics, in developing countries, the incidence rate of chronic suppurative otitis media in children is 1.3%~10.6%.